Treating Calcaneal Apophysitis
Overview
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Having flatfeet or very pronated feet can make one prone to Sever's disease. But also patient?s that have a very high arch foot structure tend to have a very high shock and high impact heel strike. This also puts extra stress on the heel and apophysis.
Symptoms
Typically, the sports injury occurs where the achilles tendon attaches to the bone. The epiphyseal growth plate is located at the end of a developing bone where cartilage turns into bone cells. As the growth center expands and unites, this area may become inflamed, causing severe pain when both sides of the heel are compressed. There is typically no swelling and no warmth, so it?s not always an easy condition to spot. The child usually has trouble walking, stiffness upon waking, and pain with activity that subsides during periods of rest.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Management by a health professional of Sever's disease is often wise. There are a few very rare problems that may be causing the pain, so a correct diagnosis is extremely important. Advice should be given on all of what is mentioned above, appropriate activity levels, the use of ice, always wearing shoes, heel raises and stretching, follow this advice. As a pronated foot is common in children with this problem, a discussion regarding the use of foot orthotics long term may be important. Strapping or tape is sometimes used during activity to limit the ankle joint range of motion. If the symptoms are bad enough and not responding to these measures, medication to help with anti-inflammatory may be needed. In some cases the lower limb may need to be put in a cast for 2-6 weeks to give it a good chance to heal. After the calcaneal apophysitis resolves, prevention with the use of stretching, good supportive shock absorbing shoe and heel raises are important to prevent it happening again.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position, If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Having flatfeet or very pronated feet can make one prone to Sever's disease. But also patient?s that have a very high arch foot structure tend to have a very high shock and high impact heel strike. This also puts extra stress on the heel and apophysis.
Symptoms
Typically, the sports injury occurs where the achilles tendon attaches to the bone. The epiphyseal growth plate is located at the end of a developing bone where cartilage turns into bone cells. As the growth center expands and unites, this area may become inflamed, causing severe pain when both sides of the heel are compressed. There is typically no swelling and no warmth, so it?s not always an easy condition to spot. The child usually has trouble walking, stiffness upon waking, and pain with activity that subsides during periods of rest.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Management by a health professional of Sever's disease is often wise. There are a few very rare problems that may be causing the pain, so a correct diagnosis is extremely important. Advice should be given on all of what is mentioned above, appropriate activity levels, the use of ice, always wearing shoes, heel raises and stretching, follow this advice. As a pronated foot is common in children with this problem, a discussion regarding the use of foot orthotics long term may be important. Strapping or tape is sometimes used during activity to limit the ankle joint range of motion. If the symptoms are bad enough and not responding to these measures, medication to help with anti-inflammatory may be needed. In some cases the lower limb may need to be put in a cast for 2-6 weeks to give it a good chance to heal. After the calcaneal apophysitis resolves, prevention with the use of stretching, good supportive shock absorbing shoe and heel raises are important to prevent it happening again.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position, If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Achilles Tendon Rupture Pain After Surgery
Overview
 Achilles tendon rupture is an injury that affects the back of your lower leg. It most commonly occurs in people playing recreational sports. The Achilles tendon is a strong fibrous cord that connects the muscles in the back of your calf to your heel bone. If you overstretch your Achilles tendon, it can tear (rupture). The tendon can rupture completely or just partially. If you have an Achilles tendon rupture, you might feel a pop or snap, followed by an immediate sharp pain in the back of your ankle and lower leg that usually affects your ability to walk properly. Surgery is often the best treatment option to repair an Achilles tendon rupture. For many people, however, nonsurgical treatment works just as well.
Achilles tendon rupture is an injury that affects the back of your lower leg. It most commonly occurs in people playing recreational sports. The Achilles tendon is a strong fibrous cord that connects the muscles in the back of your calf to your heel bone. If you overstretch your Achilles tendon, it can tear (rupture). The tendon can rupture completely or just partially. If you have an Achilles tendon rupture, you might feel a pop or snap, followed by an immediate sharp pain in the back of your ankle and lower leg that usually affects your ability to walk properly. Surgery is often the best treatment option to repair an Achilles tendon rupture. For many people, however, nonsurgical treatment works just as well.
Causes
The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms.
Symptoms
Typically patients present with sudden onset of pain and swelling in the achilles region, often accompanied by a audible snap during forceful dorsiflexion of the foot. A classic example is that of an unfit 'weekend warrior' playing squash. If complete a defect may be felt and the patient will have only minimal plantar flexion against resistance.
Diagnosis
Some patients mistakenly believe the tendon is working if they can push the foot down, however, patients will usually be able to move the foot up and down while sitting because the other surrounding muscles and tendons are still intact. Trying to push up while standing and applying body weight to the foot will reveal the true weakness. Sensation and circulation to the foot and ankle will be normal. In addition, x-rays will be normal unless the Achilles injury involves pulling off (avulsion) of the bone on the calcaneus (heel bone). This is quite rare, occurring in only a small fraction of patients with Achilles injuries. Patients suffering this type of Achilles avulsion injury tend to be older with weaker bone. Imaging Studies. Plain x-rays will be negative in patients who have suffered an Achilles tendon rupture. The rupture can be seen on ultrasound or MRI. However, these studies are not indicated for acute ruptures unless there is some uncertainty about the diagnosis. For chronic problems of the Achilles or ruptures that are old, an MRI may be very helpful.
Non Surgical Treatment
Non-operative treatment consists of placing the foot in a downward position [equinus] and providing relative immobilization of the foot in this position until the Achilles has healed. This typically involves some type of stable bracing or relative immobilization for 6 weeks, often with limited or no weight bearing. The patient can then be transitioned to a boot with a heel lift and then gradually increase their activity level within the boot. It is very important that the status of the Achilles is monitored throughout non-operative treatment. This can be done by examination or via ultrasound. If there is evidence of gapping or non-healing, surgery may need to be considered. Formal protocols have been developed to help optimize non-operative treatments and excellent results have been reported with these protocols. The focus of these treatments is to ensure that the Achilles rupture is in continuity and is healing in a satisfactory manner. The primary advantage of non-operative treatment is that without an incision in this area, there are no problems with wound healing or infection. Wound infection following Achilles tendon surgery can be a devastating complication and therefore, for many patients, non-operative treatment should be contemplated. The main disadvantage of non-operative treatment is that the recovery is probably slower. On average, the main checkpoints of recovery occur 3-4 weeks quicker with operative treatment than with non-operative treatment. In addition, the re-rupture rate appears to be higher with some non-operative treatments. Re-rupture typically occurs 8-18 months after the original injury. 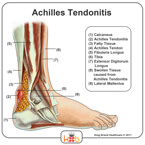
Surgical Treatment
Surgery could allow for a quicker healing time. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the tissue, the repair may be reinforced with other tendons. As with any surgery, the main complication is the risk for infection, however, this risk is reduced by using smaller incisions.
Prevention
The following can significantly reduce the risk of Achilles tendon rupture. Adequate stretching and warming up prior to exercising. If playing a seasonal sport, undertake preparatory exercises to build strength and endurance before the sporting season commences. Maintain a healthy body weight. This will reduce the load on the tendon and muscles. Use footwear appropriate for the sport or exercise being undertaken. Exercise within fitness limits and follow a sensible exercise programme. Increase exercise gradually and avoid unfamiliar strenuous exercise. Gradual ?warm down? after exercising.
Leg Length Discrepancy Shoe Lift
Overview
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
Some causes of leg length discrepancy (other than anatomical). Dysfunction of the hip joint itself leading to compensatory alterations by the joint and muscles that impact on the joint. Muscle mass itself, i.e., the vastus lateralis muscle, pushes the iliotibial band laterally, causing femoral compensations to maintain a line of progression during the gait cycle. This is often misdiagnosed as I-T band syndrome and subsequently treated incorrectly. The internal rotators of the lower limb are being chronically short or in a state of contracture. According to Cunningham's Manual of Practical Anatomy these are muscles whose insertion is lateral to the long axis of the femur. The external rotators of the hip joint are evidenced in the hip rotation test. The iliosacral joint displays joint fixations on the superior or inferior transverse, or the sagittal axes. This may result from many causes including joint, muscle, osseous or compensatory considerations. Short hamstring muscles, i.e., the long head of the biceps femoris muscle. In the closed kinetic chain an inability of the fibula to drop inferior will result in sacrotuberous ligament loading failure. The sacroiliac joint dysfunctions along its right or left oblique axis. Failure or incorrect loading of the Back Force Transmission System (the longitudinal-muscle-tendon-fascia sling and the oblique dorsal muscle-fascia-tendon sling). See the proceedings of the first and second Interdisciplinary World Congress on Low Back Pain. Sacral dysfunction (nutation or counternutation) on the respiratory axis. When we consider the above mentioned, and other causes, it should be obvious that unless we look at all of the causes of leg length discrepancy/asymmetry then we will most assuredly reach a diagnosis based on historical dogma or ritual rather than applying the rules of current differential diagnosis.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
Treatments for limb-length discrepancies and differences vary, depending on the cause and severity of the condition. At Gillette, our orthopedic surgeons are experts in typical and atypical growth and development. Our expertise lets us plan treatments that offer a lifetime of benefits. Treatments might include monitoring growth and development, providing noninvasive treatments or therapy, and providing a combination of orthopedic surgical procedures. To date, alternative treatments (such as chiropractic care or physical therapy) have not measurably altered the progression of or improved limb-length conditions. However, children often have physical or occupational therapy to address related conditions, such as muscle weakness or inflexibility, or to speed recovery following a surgical procedure. In cases where surgical treatment isn?t necessary, our orthopedists may monitor patients and plan noninvasive treatments, such as, occupational therapy, orthoses (braces) and shoe inserts, physical therapy, prostheses (artificial limbs).

Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
Some causes of leg length discrepancy (other than anatomical). Dysfunction of the hip joint itself leading to compensatory alterations by the joint and muscles that impact on the joint. Muscle mass itself, i.e., the vastus lateralis muscle, pushes the iliotibial band laterally, causing femoral compensations to maintain a line of progression during the gait cycle. This is often misdiagnosed as I-T band syndrome and subsequently treated incorrectly. The internal rotators of the lower limb are being chronically short or in a state of contracture. According to Cunningham's Manual of Practical Anatomy these are muscles whose insertion is lateral to the long axis of the femur. The external rotators of the hip joint are evidenced in the hip rotation test. The iliosacral joint displays joint fixations on the superior or inferior transverse, or the sagittal axes. This may result from many causes including joint, muscle, osseous or compensatory considerations. Short hamstring muscles, i.e., the long head of the biceps femoris muscle. In the closed kinetic chain an inability of the fibula to drop inferior will result in sacrotuberous ligament loading failure. The sacroiliac joint dysfunctions along its right or left oblique axis. Failure or incorrect loading of the Back Force Transmission System (the longitudinal-muscle-tendon-fascia sling and the oblique dorsal muscle-fascia-tendon sling). See the proceedings of the first and second Interdisciplinary World Congress on Low Back Pain. Sacral dysfunction (nutation or counternutation) on the respiratory axis. When we consider the above mentioned, and other causes, it should be obvious that unless we look at all of the causes of leg length discrepancy/asymmetry then we will most assuredly reach a diagnosis based on historical dogma or ritual rather than applying the rules of current differential diagnosis.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
Treatments for limb-length discrepancies and differences vary, depending on the cause and severity of the condition. At Gillette, our orthopedic surgeons are experts in typical and atypical growth and development. Our expertise lets us plan treatments that offer a lifetime of benefits. Treatments might include monitoring growth and development, providing noninvasive treatments or therapy, and providing a combination of orthopedic surgical procedures. To date, alternative treatments (such as chiropractic care or physical therapy) have not measurably altered the progression of or improved limb-length conditions. However, children often have physical or occupational therapy to address related conditions, such as muscle weakness or inflexibility, or to speed recovery following a surgical procedure. In cases where surgical treatment isn?t necessary, our orthopedists may monitor patients and plan noninvasive treatments, such as, occupational therapy, orthoses (braces) and shoe inserts, physical therapy, prostheses (artificial limbs).
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Acquired Flat Foot Tibialis Posterior Tenosynovitis
Overview
Often considered solely a product of genetics, flatfoot rarely carries with it the stigma of presenting over time. The truth, however, is that flatfoot does not discriminate on the basis of age and can become an issue in the form of adult-acquired flatfoot. Like its congenital cousin, adult-acquired flatfoot deformity is one that, in causing structural damage to the foot (and particularly to the posterior tibial tendon), creates an imbalance that may result in any number of symptoms, including inflammation, pain, stiffness, limited mobility, and even arthritis. 
Causes
The cause of posterior tibial tendon insufficiency is not completely understood. The condition commonly does not start from one acute trauma but is a process of gradual degeneration of the soft tissues supporting the medial (inner) side of the foot. It is most often associated with a foot that started out somewhat flat or pronated (rolled inward). This type of foot places more stress on the medial soft tissue structures, which include the posterior tibial tendon and ligaments on the inner side of the foot. Children nearly fully grown can end up with flat feet, the majority of which are no problem. However, if the deformity is severe enough it can cause significant functional limitations at that age and later on if soft tissue failure occurs. Also, young adults with normally aligned feet can acutely injure their posterior tibial tendon from a trauma and not develop deformity. The degenerative condition in patients beyond their twenties is different from the acute injuries in young patients or adolescent deformities, where progression of deformity is likely to occur.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found. 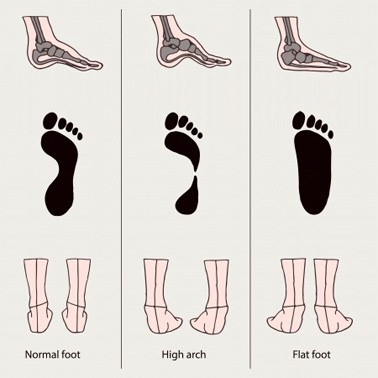
Surgical Treatment
Flatfoot reconstruction (osteotomy). This is often recommended for flexible flatfoot condition. Flatfoot reconstruction involves cutting and shifting the heel bone into a more neutral position, transferring the tendon used to flex the lesser toes (all but the big toe) to strengthen the posterior tibial tendon, and lengthening the calf muscle. Fusion (also known as triple arthrodesis). Fusion involves fusing, or making stiff, three joints in the back of the foot the subtalar, talonavicular, and calcaneocuboid joints, to realign the foot and give it a more natural shape. Pins or screws hold the area in place until it heals. Fusion is often recommended for a rigid flatfoot deformity or evidence of arthritis. Both of these surgeries can provide excellent pain relief and correction.
The Causes And Treatments
Overview
Adult acquired flatfoot deformity (AAFD) is a painful, chronic condition found most often in women between the ages of 40 and 60. AAFD occurs when the soft tissues of the foot are overstretched and torn, causing the arch to collapse. Flatfoot deformities may also be caused by a foot fracture, or may result from long-term arthritis. Once the posterior tibial tendon-the tendon unit that holds up the arch-loses its function, the foot becomes ?flat? as the bones spread out of position during weight bearing. Without an AAFD repair, the condition may progress until the affected foot becomes entirely rigid and quite painful. 
Causes
The posterior tibial tendon, which connects the bones inside the foot to the calf, is responsible for supporting the foot during movement and holding up the arch. Gradual stretching and tearing of the posterior tibial tendon can cause failure of the ligaments in the arch. Without support, the bones in the feet fall out of normal position, rolling the foot inward. The foot's arch will collapse completely over time, resulting in adult acquired flatfoot. The ligaments and tendons holding up the arch can lose elasticity and strength as a result of aging. Obesity, diabetes, and hypertension can increase the risk of developing this condition. Adult acquired flatfoot is seen more often in women than in men and in those 40 or older.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. 
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Will Posterior Tibial Tendon Dysfunction (PTTD) Always Involve Surgical Pocedures ?
Overview Flatfoot may sound like a characteristic of a certain water animal rather than a human problem. Flatfoot is a condition in which the arch of the foot is fallen and the foot is pointed outward. In contrast to a flatfoot condition that has always been present, this type develops after the skeleton has reached maturity. There are several situations that can result in fallen arches, including fracture, dislocation, tendon laceration, tarsal coalition, and arthritis. One of the most common conditions that can lead to this foot problem is posterior tibial tendon dysfunction. The posterior tibial tendon attaches the calf muscle to the bones on the inside of the foot and is crucial in holding up and supporting the arch. An acute injury or overuse can cause this tendon to become inflamed or even torn, and the arch of the foot will slowly fall over time.  Causes As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem. Symptoms Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop. Diagnosis Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot. Non surgical Treatment Treatment will vary depending on the degree of your symptoms. Generally, we would use a combination of rest, immobilization, orthotics, braces, and physical therapy to start. The goal is to keep swelling and inflammation under control and limit the stress on the tendon while it heals. Avoidance of activities that stress the tendon will be necessary. Once the tendon heals and you resume activity, physical therapy will further strengthen the injured tendon and help restore flexibility. Surgery may be necessary if the tendon is torn or does not respond to these conservative treatment methods. Your posterior tibial tendon is vital for normal walking. When it is injured in any way, you risk losing independence and mobility. Keep your foot health a top priority and address any pain or problems quickly. Even minor symptoms could progress into chronic problems, so don?t ignore your foot pain.
Causes As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem. Symptoms Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop. Diagnosis Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot. Non surgical Treatment Treatment will vary depending on the degree of your symptoms. Generally, we would use a combination of rest, immobilization, orthotics, braces, and physical therapy to start. The goal is to keep swelling and inflammation under control and limit the stress on the tendon while it heals. Avoidance of activities that stress the tendon will be necessary. Once the tendon heals and you resume activity, physical therapy will further strengthen the injured tendon and help restore flexibility. Surgery may be necessary if the tendon is torn or does not respond to these conservative treatment methods. Your posterior tibial tendon is vital for normal walking. When it is injured in any way, you risk losing independence and mobility. Keep your foot health a top priority and address any pain or problems quickly. Even minor symptoms could progress into chronic problems, so don?t ignore your foot pain.  Surgical Treatment For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both.
Surgical Treatment For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both.